

Spring Issue Articles

Kate White, MA,
BCBMT, RCST®, CEIM, SEP, PPNE
There is a saying in osteopathy, “As the twig is bent, so grows the tree.†What we mean by that is, if a small tree is somehow affected in its growth sequence, it might follow that growth pattern into its prime. Imagine a young tree affected by wind, weather, or injury, then growing again but at an angle or with a large burl. Seeing humans as trees is a way to talk about prenatal and birth trauma as part of the earliest development of a baby, the root of the tree. The roots form the basis for the rest of the tree, with birth at the ground level, early childhood in the trunk, adolescence in the branches and adulthood in the canopy. In earliest trauma, during the prenatal and perinatal time, we can track layers and sequences connected to these earliest experiences.
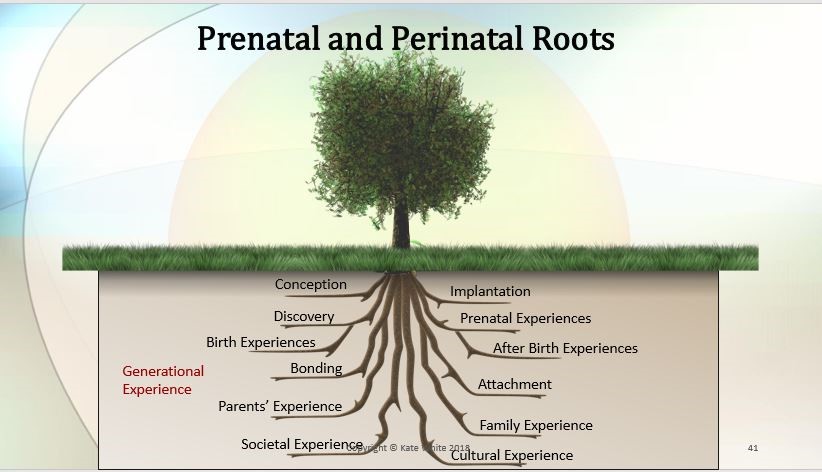 The soil around the roots can be labeled as our intergenerational/ transgenerational genetic material. Our ancestors are part of our inheritance. Research has shown that trauma can cross generations such as the impact of famine, war, or natural disaster. Trauma can travel from parent to child in learned behaviors. As you can see in this picture, there are many layers in the prenatal and perinatal period:
The soil around the roots can be labeled as our intergenerational/ transgenerational genetic material. Our ancestors are part of our inheritance. Research has shown that trauma can cross generations such as the impact of famine, war, or natural disaster. Trauma can travel from parent to child in learned behaviors. As you can see in this picture, there are many layers in the prenatal and perinatal period:
- Conception
- Implantation
- Discovery of the pregnancy (the Little One!) 1
- Prenatal experiences, like twin dynamics
- Birth experiences, like use of interventions, long or fast births
- After birth experiences, like separations, stays in the neonatal intensive care
- Bonding and attachment, are there any ruptures?
- Parent experiences, like birth trauma or postpartum depression
- Family experiences, including having little or no support, siblings too close in age
- Societal and cultural experiences, like rules around numbers of or gender of children
There are indicators for each of the layers that show up if the story is still there, cycling around waiting for healing conditions. Here are some conditions that might occur where healing wants to happen in the prenatal and perinatal realm:
-
- Conception is a vital time in human development; best outcomes are when couples are consciously inviting a baby in. But data show that almost half of pregnancies are mistimed or unwanted. For the incoming human being who is not wanted or welcomed, healing lies in opportunities to feel wanted in present time. The Little One asks, Am I wanted? Am I welcomed? A nurturing healing message for conception can be: I am waiting for you, I am watching for you. When a baby is wanted, the mother waits for the good news.
-
- Implantation patterns are connected to finding and making a home. How are moving transitions for you? They can be very stressful. How was your last move for you? Did you notice any feelings of depression or high anxiety? Or were you excited? Was finding, moving and creating a new home easy for you? These are all connections to when the Little One finds a place to implant in the womb. And how is it to be discovered? In prenatal and perinatal healing, we know that if a baby is not wanted on discovery of pregnancy, it can be shocking.
-
- There are many prenatal experiences that a baby might encounter in relationship to their mother’s experiences, or in very impersonal anatomical and developmental issues. Recent research suggests that babies feel their body through movement in utero, and it islinked to a sense of self. David Chamberlain, author of Windows to the Womb: Revealing the Conscious Baby from Conception to Birth, and co-founder of the Association for Prenatal and Perinatal Psychology and Health claimed that babies have 12 senses in utero, not just five, and these senses feed human consciousness. The roots of how we feel about ourselves start in utero, as do many epigenetic challenges. If a mother experiences toxic stress so does the baby.
-
- Birth interventions can have an equally large imprint on a baby’s experience. If we need to be helped at birth, it often hurts but helps, too. A feeling of a double bind can arise, where the person feels like if they do nothing, it hurts (or worse, they feel like they are going to die), but if they get help, it will hurt, too. This can be like a Little One who is stuck in utero and needs help to be born.
Bonding and attachment are some of the most studied research patterns in human development. Research shows that attachment patterns can cross generations, so that a parent can unconsciously parent their children like they were parented. We know that secure attachment helps create better health on every level: cognitive, emotional, physical, mental and spiritual. It lays the groundwork for health lifelong, especially in relationships. Bonding and attachment starts in the womb, and even preconception.
These are but a few of the patterns that can be addressed by understanding what happens during the first months and years of life. Professionals can gain skills in working with earliest trauma, especially somatic specialists like Somatic Experiencing® practitioners or those trained in somatic psychology. Skills that help integrate our earliest experiences include:
-
-
- Slowing
- Noticing sensation and gesture, what is the nonverbal story?
- Allow space for the story to unfold in the body, since it is an implicit, somatic memory.
- Self and co-regulation with
- Listen for metaphors in language and
- Are there patterns that occur over and over? We see this most often in double
- Differentiation is key to help uncouple past from
- The best of Somatic Experiencing comes into play: titration and pendulation, but with earliest trauma, the practitioner will need to be ready for big survival energy and even terror, as many early patterns have near death experiences coupled with them.
-
Learning about healing our earliest trauma can start with simple explorations in books, or in the online classes offered by the Association for Prenatal and Perinatal Psychology and Health (APPPAH). Basic practitioner skills are offered in the new ‘Toolkits for Facilitators’, or in the on-demand classes. To see more about APPPAH, go to birthpsychology.com or our new online Classwomb™ http://www.birth-psychology- teachable.com. Lectures and experiential classes are offered through my center, the Center for Prenatal and Perinatal Programs.
1 In the language of understanding earliest imprints, or the layers of implicit memory in our bodies from the prenatal and birth time, we refer to who we are at this as the Little One. Some practitioners also call this experience the Baby Self, or even, Little Poopsie (hat tip, Franklyn Sills!)
Kate White is an award-winning prenatal and perinatal educator and an advanced bodyworker. She is trained in somatic therapies, prenatal and perinatal health, lactation, brain development, infant mental health, and has specialized in mother-baby dyad care using somatic prevention and trauma healing approaches for nearly 20 years. She is a mother of two children, holds a BA and MA in Communication, a Registered Craniosacral Therapist in the Biodynamic Craniosacral method and a Somatic Experiencing® Practitioner. Her work combines somatic therapy, birth preparation, recovery from difficult birth, trauma resolution and brain development to help give families with babies and small children the best possible start. She is the Founding Director of Education for the Association for Prenatal and Perinatal Psychology and Health and currently co-directs this department, administering an online program for parents and parent professionals, runs a private practice and offers her own seminars through the Center for Prenatal and Perinatal Programs. www.ppncenter.com




